Elderly Mortality After Trauma
Published in academic literature
App Summary
App Screenshots
Detailed Description
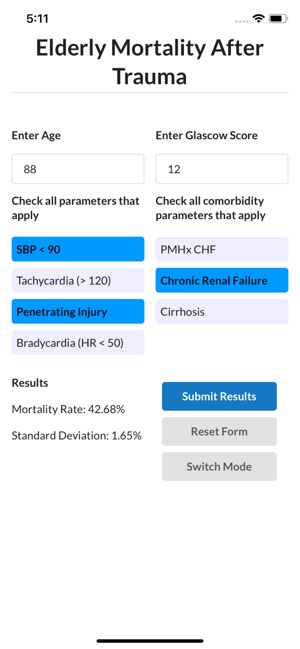
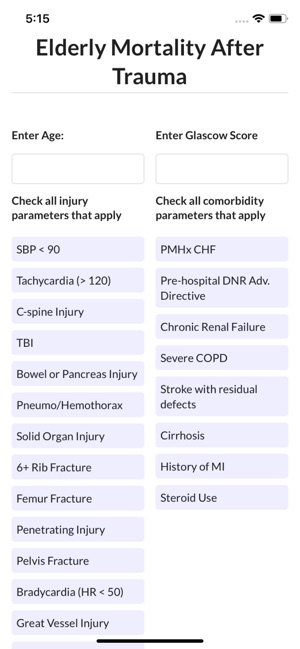
Functionality & Mechanism
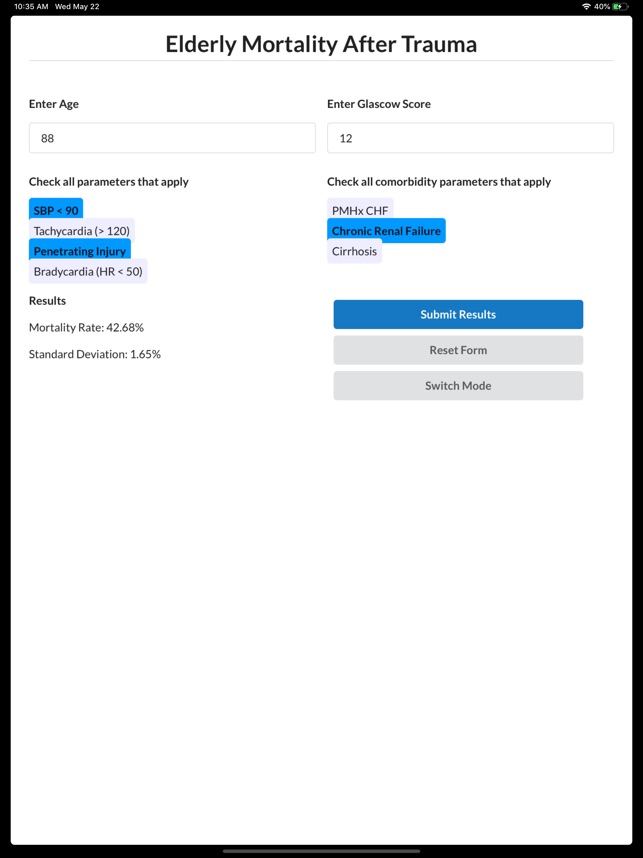
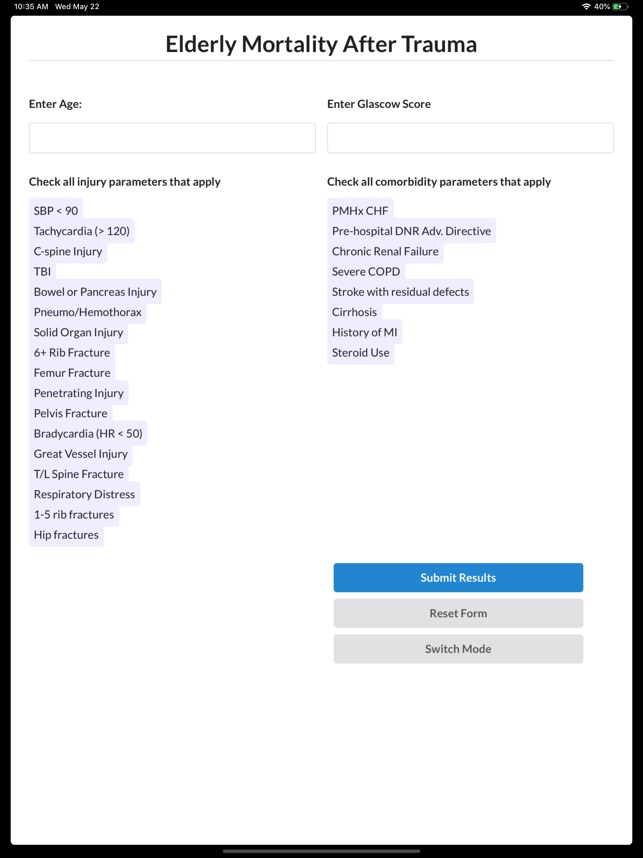
The Elderly Mortality After Trauma (EMAT) system calculates the probability of in-hospital mortality for geriatric trauma patients. The interface facilitates risk assessment via two distinct modules: a rapid Quick (qEMAT) score for initial presentation and a comprehensive Full (fEMAT) score for use after radiologic evaluation. The system captures input on patient age, comorbidities, physiologic parameters, and injury types to generate a predictive score, with the full module leveraging 26 factors for enhanced accuracy.
Evidence & Research Context
- The EMAT scoring system was developed and validated in a large-scale epidemiological study using National Trauma Databank records from over 1.2 million patients aged 65 and older.
- A validation study (N=427,358) demonstrated strong discrimination for predicting in-hospital mortality, with an Area Under the Curve (AuROC) of 0.86 for the fEMAT and 0.84 for the qEMAT.
- The fEMAT model was shown to outperform other standard trauma mortality prediction tools, including the Trauma and Injury Severity Score (TRISS) and age plus Injury Severity Score (ISS).
- In a comparative analysis using a regional trauma registry, the qEMAT model demonstrated superior predictive performance over the Geriatric Trauma Outcome Score (GTOS).
Intended Use & Scope
This clinical reference tool is intended for physicians and trauma care teams. Its primary utility is to provide rapid, data-driven mortality risk stratification to inform decisions regarding patient transfers, family counseling, and palliative care consultation. The scores estimate in-hospital mortality only and are not a substitute for comprehensive clinical judgment or a predictor of long-term outcomes.
Studies & Publications
Peer-reviewed research associated with this app.
Predictors of elderly mortality after trauma: A novel outcome score
Morris et al. (2020) · Journal of Trauma and Acute Care Surgery
Describes the research-driven development of this appApp Information
Developer
University of MinnesotaCategory
Evidence Profile
Published in academic literature
Platforms
Updated
Nov 2019
© 2025 University of Minnesota
Tags
Developer Links
Privacy PolicyElderly Mortality After Trauma
Free