HeRS - Hemorrhage Risk Stratification Calculator
Published in academic literature
App Summary
App Screenshots

Detailed Description
Functionality & Mechanism
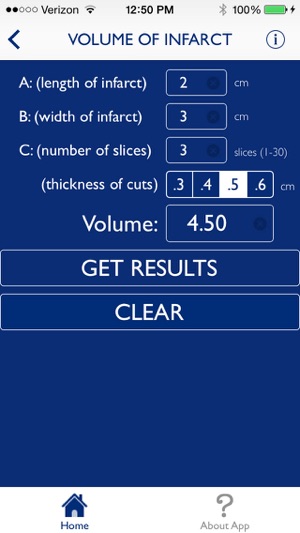
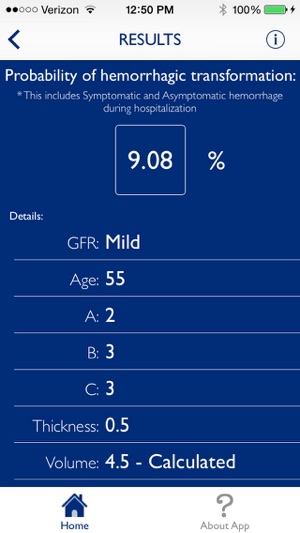
HeRS is a clinical calculator designed for rapid risk stratification. The system quantifies the probability of hemorrhagic transformation in patients with acute ischemic stroke who have an indication for anticoagulation. The interface captures continuous variables for patient age, renal function (eGFR), and infarct volume. It then leverages a complex, prospectively validated regression equation to compute the HeRS score, delivering a precise risk assessment in seconds to circumvent the difficulty of manual calculation in a clinical setting.
Evidence & Research Context
- A prospective validation study (N=241) conducted at two academic stroke centers established the HeRS score as a valid predictor of hemorrhagic transformation, demonstrating a predictive accuracy (AUC) of 0.701.
- The same validation study identified that incorporating serum glucose, white blood cell count, and prior warfarin use into the model enhanced predictive accuracy, increasing the AUC to 0.854.
- The score's core variables were derived from a retrospective analysis (N=123) that identified age, infarct volume, and eGFR as significant, independent predictors of hemorrhagic events in this patient population.
- Initial research noted that while anticoagulation did not significantly increase overall hemorrhage rates, all observed intracerebral hematomas and symptomatic hemorrhages occurred within the anticoagulated patient group.
Intended Use & Scope
This tool is intended for clinicians managing acute ischemic stroke care, including neurologists and hospitalists. Its primary utility is as a clinical decision support instrument to inform discussions and decisions regarding the initiation of anticoagulation therapy. The calculator provides a specific risk probability and does not replace comprehensive clinical judgment or patient-specific factors.
Studies & Publications
Peer-reviewed research associated with this app.
Predicting Hemorrhagic Transformation of Acute Ischemic Stroke: Prospective Validation of the HeRS Score
Marsh et al. (2016) · Medicine
Referenced in academic literature; no direct evaluation of the appThe association between specific substances of abuse and subcortical intracerebral hemorrhage versus ischemic lacunar infarction
Kaplan et al. (2014) · Frontiers in Neurology
Referenced in academic literature; no direct evaluation of the appApp Information
Developer
Johns Hopkins UniversityCategory
Evidence Profile
Published in academic literature
Platforms
Updated
Dec 2014
© 2025 Johns Hopkins University
Tags
HeRS - Hemorrhage Risk Stratification Calculator
Free