Pediatric Asthma Risk Score
Published in academic literature
App Summary
App Screenshots

Detailed Description
Functionality & Mechanism
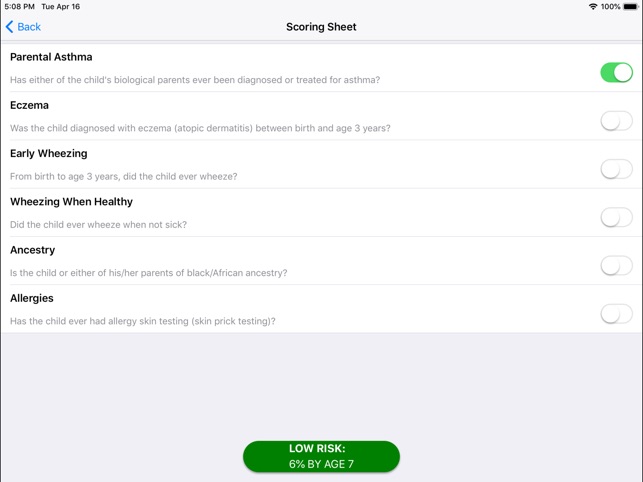
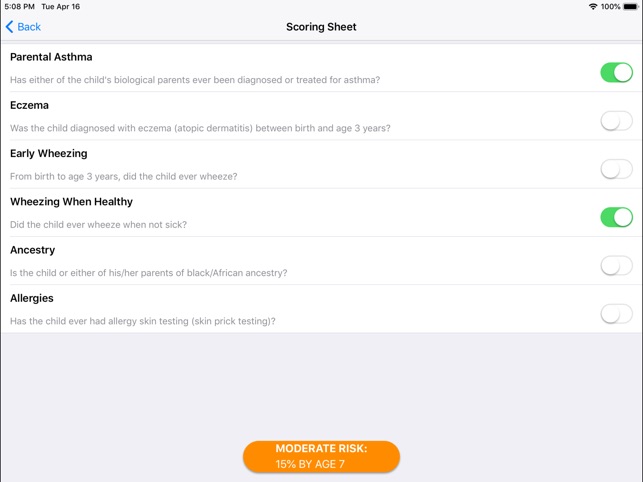
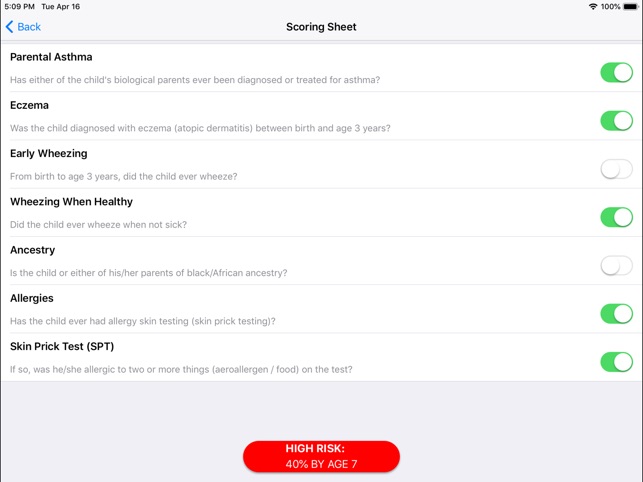
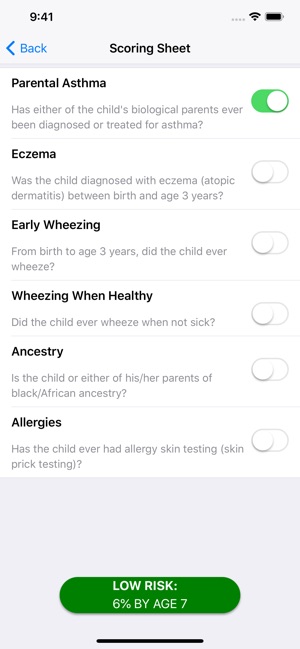
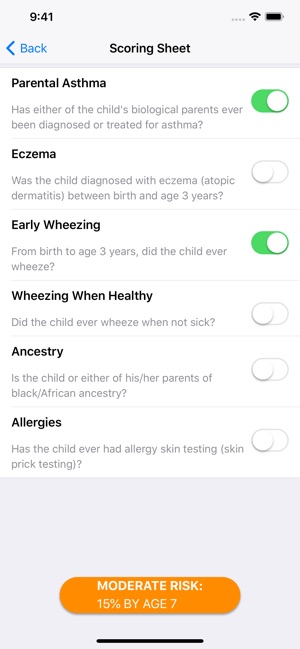
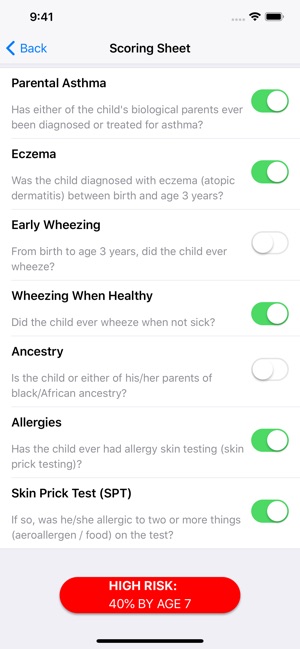
Developed at Cincinnati Children's Hospital Medical Center, the Pediatric Asthma Risk Score (PARS) is a clinical calculation tool that generates a personalized asthma risk score for young children. The interface captures input on six weighted risk factors: parental asthma, eczema, wheezing history, allergen sensitization, and race. The system processes these inputs to yield a continuous score from 0 to 14, corresponding to a specific percentage risk of developing asthma by age seven.
Evidence & Research Context
- The PARS model was developed and validated in a large birth cohort (N=762) and its performance was successfully replicated in a second, independent international cohort, demonstrating robust and generalizable predictive accuracy.
- Across cohorts, the tool demonstrated strong performance metrics, with sensitivity ranging from 0.67–0.68 and specificity from 0.77–0.79 for predicting asthma development by age seven.
- Compared to the widely used Asthma Predictive Index (API), the PARS provides an 11% increase in sensitivity and shows superior capability in identifying children with mild-to-moderate risk.
- Key predictive factors incorporated into the weighted score include early wheezing (OR 2.88), sensitization to multiple allergens (OR 2.44), and African American race (OR 2.04).
Intended Use & Scope
Designed for clinicians, PARS functions as a point-of-care screening tool to quantify a young child's future asthma risk. The score is intended to facilitate risk stratification and parental counseling. It is not a diagnostic instrument and does not provide clinical management recommendations; further clinical evaluation is required for diagnosis and treatment.
Studies & Publications
Peer-reviewed research associated with this app.
The pediatric asthma risk score (PARS): making the move to the most accurate pediatric asthma risk screening tool
Sherenian et al. (2019) · Expert Review of Clinical Immunology
Referenced in academic literature; no direct evaluation of the appA Pediatric Asthma Risk Score (PARS) to Better Predict Asthma Development in Young Children
Biagini Myers et al. (2019) · Journal of Allergy and Clinical Immunology
Referenced in academic literature; no direct evaluation of the appApp Information
Category
Evidence Profile
Published in academic literature
Platforms
Updated
Apr 2019
© 2025 Cincinnati Children's Hospital Medical Center
Tags
Developer Links
Privacy PolicyPediatric Asthma Risk Score
Free