Mindfulness and Sickle Cell
Validated in clinical trials · Initial evidence
App Summary
App Screenshots

Detailed Description
Functionality & Mechanism
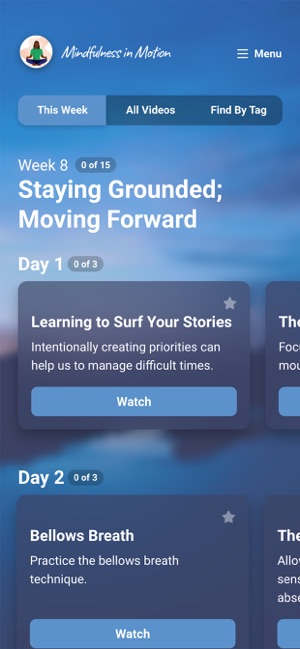
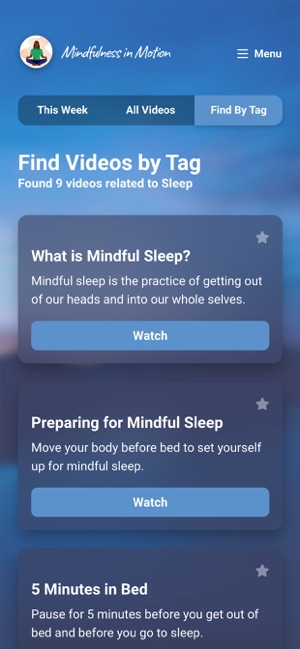
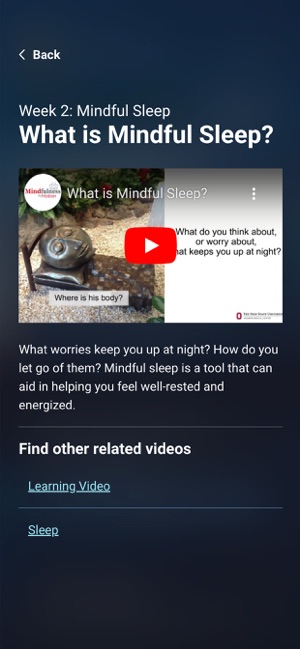
Developed for individuals with sickle cell disease (SCD), this system delivers mindfulness-based self-management strategies through a mobile interface. The platform provides access to a library of over 120 educational videos, guided meditations, and gentle stretching routines designed to impart physical and mental coping skills. Users select content based on their needs, and the system monitors engagement through video completion records and brief integrated surveys, facilitating progress tracking and reinforcing the application of mindfulness principles in daily life.
Evidence & Research Context
- Associated research posits that a biopsychosocial model, which incorporates neurologic and psychological factors, is required for the effective management of chronic pain in sickle cell disease (SCD).
- The authors propose mindfulness-based pain management training as a core component of this model to help individuals recognize pain triggers and modulate emotional and physical responses.
- The app's intervention model is informed by research on 'Mindfulness in Motion,' a preliminary trial of which demonstrated feasibility (97% retention) and significant increases in resiliency in a non-SCD, high-stress population.
Intended Use & Scope
This tool is designed for individuals with sickle cell disease as an adjunct therapy for self-managing the psychosocial and physical challenges of the condition. It delivers supportive educational content but does not provide medical advice or replace clinical care, including prescribed pharmacotherapy. The app should be utilized in consultation with a healthcare professional as part of a comprehensive treatment plan.
Studies & Publications
Peer-reviewed research associated with this app.
Treating Chronic Pain in Sickle Cell Disease — The Need for a Biopsychosocial Model
Childerhose et al. (2023) · New England Journal of Medicine
Referenced in academic literature; no direct evaluation of the appMindfulness in Motion (MIM): An Onsite Mindfulness Based Intervention (MBI) for Chronically High Stress Work Environments to Increase Resiliency and Work Engagement
Klatt et al. (2015) · Journal of Visualized Experiments
Improved work engagement and resiliency compared to control group in high-stress workplace environments.
App Information
Developer
Ohio State UniversityCategory
Evidence Profile
Validated in clinical trials · Initial evidence
Platforms
Updated
Nov 2025
© 2025 Ohio State University